The Operational Case for Portable X-Ray in Occupational Medicine
The Operational Case for Portable X-Ray in Occupational Medicine
Faster diagnoses, fewer disputes, better workflow — why on-site imaging is reshaping occ-med clinic economics.
Occupational medicine clinics face a unique imaging challenge: the patient is rarely the customer. Employers, insurers, and case managers all watch the clock — and on-site portable X-ray has quietly become one of the highest-leverage operational upgrades an occ-med practice can make. Here is the practical case.
Occupational medicine sits at the intersection of healthcare and human resources. Every imaging decision — when, where, by whom — shows up downstream in three places at once: a worker’s recovery, an employer’s lost-time exposure, and a workers’ compensation file. Owning that imaging step on-site, with portable X-ray equipment, changes the economics of all three.
For occ-med clinic operators, the question is no longer whether portable imaging belongs in the practice — it’s how quickly the operational upside can be captured. This article walks through the practical, dollars-and-workflow benefits of bringing portable X-ray in-house.
Why occupational medicine is structurally different
A standard urgent-care patient walks in, gets a diagnosis, and goes home. An occ-med patient is rarely that simple. Behind every visit there are typically three additional stakeholders: an employer waiting on a fitness-for-duty determination, a workers’ comp carrier waiting on documentation, and (for DOT, FAA, OSHA-recordable, or pre-employment cases) a regulatory clock.
That structure changes what “good imaging” looks like. Speed of result, defensibility of documentation, and continuity of the patient encounter become as important as image quality itself. Sending a patient down the street to a hospital radiology department fragments all three.
Benefit 1: Same-visit diagnosis collapses the return-to-work timeline
The single biggest economic lever in workers’ compensation is time-to-disposition. Every day a worker is in limbo — not yet cleared, not yet on modified duty, not yet referred — is a day of indemnity exposure for the employer and uncertainty for the worker.
On-site portable X-ray converts what would otherwise be a multi-day diagnostic loop (clinic visit → outside imaging referral → follow-up appointment) into a single encounter. The provider examines the worker, captures the image, reviews it during the same visit, and issues a return-to-work determination before the patient leaves. Industry guidance from workers’ compensation specialists notes that timely diagnostic imaging directly accelerates treatment decisions and shortens absences (Enlyte).
For a clinic seeing 20–40 occupational injury cases per week, compressing even a single day from each return-to-work timeline is a measurable win for the employer relationships that drive occ-med revenue.
Benefit 2: Stronger claims documentation, fewer disputes
Workers’ compensation cases that get disputed almost always come down to documentation gaps: was the injury work-related, what was the actual severity, did the recommended treatment match the finding? Imaging captured at the moment of presentation — with the clinic’s own equipment, in the clinic’s own record — is the highest-quality evidence a provider can produce.
Per workers’ compensation industry analysis, accurate diagnostic imaging directly supports claim validation, reduces disputes, and speeds case processing for both employees and payers (Enlyte). On-site portable X-ray also keeps the chain of custody clean: the same provider who examined the worker also captured and reviewed the image, with consistent timestamps and a single chart entry.
Benefit 3: A new revenue line that earns its keep quickly
In most occ-med settings, X-ray is a billable service — either through workers’ compensation, employer direct contracts, or third-party payers for non-injury exams (pre-employment physicals, DOT certifications, return-from-leave clearance). When the imaging would have been outsourced anyway, bringing it in-house converts an outflow (referral fees, patient inconvenience, follow-up overhead) into an inflow.
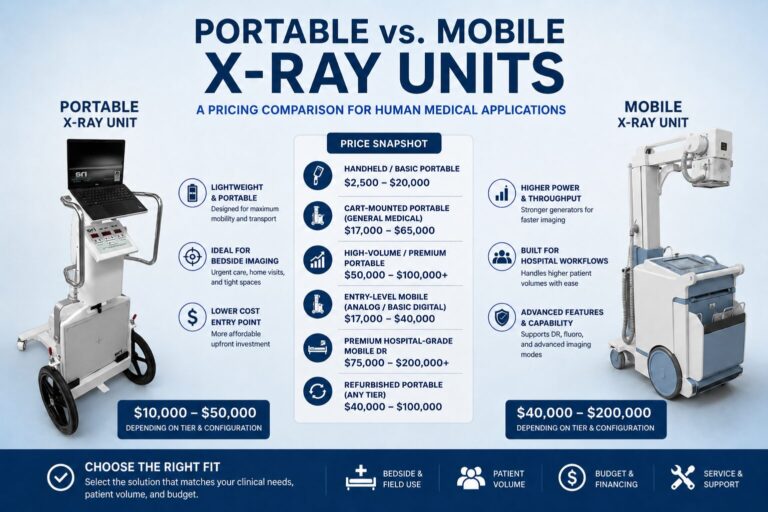
A modern portable handheld unit or compact mobile DR system can be deployed for a fraction of what a fixed radiography room would cost, and many clinics report payback periods measured in months rather than years. The unit is also redeployable: you can use it across multiple exam rooms, take it into a satellite location, or bring it to an employer’s facility for an on-site clinic day.
Benefit 4: Better throughput in the rooms that drive occ-med revenue
Occupational medicine clinics live or die on throughput per provider hour. The traditional imaging workflow — walk the patient down the hall, hand off to a tech, walk them back, wait for the read — stalls the exam room. Portable systems flip the model: the equipment comes to the patient. The provider keeps the room turning.
For employers running OSHA-driven post-incident assessments or batch pre-employment physicals (a fleet hire, a seasonal ramp, a new construction crew), this throughput advantage compounds. A clinic that can run 30 employees through a coordinated battery — vitals, vision, hearing, drug screen, and X-ray — in a single morning becomes the obvious vendor for the contract.
Benefit 5: Going to the work site, not the other way around
Portability’s most underrated benefit is geographic reach. With a battery-capable unit, an occ-med practice can run on-site clinic days at warehouses, manufacturing plants, construction sites, agricultural operations, and large employer campuses. Every employee imaged on-site is one fewer who has to leave the job for a half-day round-trip.
For employers, the math is straightforward: the wage cost of a worker traveling to a clinic and waiting in a queue almost always exceeds the per-employee cost of bringing the clinic to them. Practices that can offer this service in their service-area pitch separate themselves quickly from clinic-bound competitors.
Benefit 6: Cleaner OSHA recordability decisions
OSHA explicitly notes that diagnostic procedures, including X-rays, do not by themselves trigger recordability under 29 CFR 1904.7 (OSHA Standard Interpretation, 2004). That rule has a practical implication: X-ray is the right tool to confirm or rule out a finding without escalating a case from first-aid into a recordable one.
When the provider can image immediately, they can make the recordability call on facts — not on guesswork — and document that decision in the chart. Employers value occ-med partners who get this category of decision right consistently. (Note: this is a workflow benefit, not legal advice. Final OSHA recordability determinations always belong to the employer’s safety team and counsel.)
Where portable X-ray realistically fits in occ-med
The strongest fit is the work that defines occupational medicine itself: extremity injuries (hand, wrist, foot, ankle), suspected fractures from slips/trips/falls, contusions and sprains where imaging clears the differential, post-incident chest imaging where indicated, and the imaging components of pre-employment, return-to-duty, DOT, and FAA exams.
It is not a substitute for hospital-grade fluoroscopy, CT, or MRI — and it shouldn’t be marketed that way. The role of portable X-ray in occ-med is to handle the high-volume, high-frequency cases that already come through the door, in the same encounter, with diagnostic-grade image quality.
What to look for in a unit
- Form factor matched to use: ultra-light handheld units excel at intra-clinic mobility and field deployment; compact mobile DR systems on a cart shine in higher-volume clinic settings where the unit moves room-to-room.
- Battery operation: a unit that runs untethered for a full clinic day (or a full on-site visit at an employer location) is far more flexible than one that always needs to be plugged in.
- Modern flat-panel DR detector: cesium iodide (CsI) detectors with ISS-class technology deliver high DQE at low dose — important for pediatric or repeat-imaging cases.
- Workflow integration: wireless image transmission to PACS or to the clinic EMR, dose tracking, and a clean technologist console reduce administrative friction.
- Image processing that reduces dose: features like virtual-grid processing can cut dose meaningfully on grid-less exposures — valuable in any clinic that re-images frequently.
- Build for cleaning: antibacterial-coated, flat surfaces matter in a setting that runs through dozens of patients per day.
- Service & support: an occ-med clinic cannot afford extended downtime; choose a vendor with a clear service plan and parts availability in your region.
The economics, summarized
Bringing X-ray in-house is one of the few capital purchases in an occ-med practice that simultaneously reduces costs (referral leakage, patient travel, exam-room idle time), increases revenue (new billable procedure, employer-contract differentiation), and improves clinical outcomes (faster diagnosis, shorter return-to-work). The case is rarely whether to do it — it’s which configuration matches the clinic’s volume profile and employer mix.
For practices weighing handheld vs. compact mobile DR, single-clinic vs. multi-site, or workers’ comp–heavy vs. balanced payer mix, the right answer is rarely off-the-shelf. We help occ-med operators map equipment selection to their actual case mix, throughput targets, and employer-contract pipeline.
Thinking about adding portable X-ray to your occ-med practice?
We’ll help you map equipment options against your patient volume and case mix — honest guidance, no pressure.
Request a ConsultationSources & References
- 6 Benefits of Diagnostic Imaging in Workers’ Compensation — Enlyte (2024)
- OSHA Standard Interpretation: X-rays and diagnostic procedures — OSHA (2004)
- Workplace Safety Officials Provide New Guidance on Recording Musculoskeletal Injuries — Fisher Phillips (2024)
- Medical Expenses Covered by Workers’ Comp — Mar-Tay Law (2025)